

Biography
Biography: Mir Anwar
Abstract
Wilms’ tumor or nephroblastoma is the most common renal tumor in children and is associated with different congenital anomalies and syndromes. Aniridia as well as hypospadias could be indices of first mutation according to Knudson and Strong hypothesis i.e., PubMed. The name came from German surgeon Max Wilms who first described about child kidney tumor. Wilms’ tumor (WT) is affecting one in 10,000 children in average population. 75% of all tumor occur among the normal children, remaining 25% are with other syndrome or congenital other defects. The frequency of Wilms’ tumor (WT) in relatives was estimated to be less than 0.4% in sibs, 0.06% in uncles and aunts, and 0.04% in first cousins. Girls have higher risk then of boys ratio is 0.89:1. Age-WT is most common in young children; with an average age being about 3-4 years.
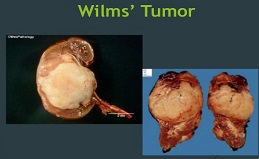
The tumor is less common in elder children and rare in adults. Race- black communities are more affected than Caucasian & Asian Communities. Mostly unilateral kidney is affected but less commonly bilateral kidney also affects. 90% of WT are unilateral, 5% are of bilateral kidney involvements. Children with WAGR syndrome have about 30% to 50% chance of having a Wilms tumor.
Birth defects like aniridia, hemi-hypertrophy, cryptorchidism, hypospadias etc. have a link of Wilms tumor. So per research has not found any strong links between WT and environmental factors either during a mother’s pregnancy or after child birth. A significant number of studies in genetics and molecular biology have improved our understanding of this malignancy discovering as well how different genes play a critical role in the organogenesis process. Surgery is obvious followed by chemotherapy. Recent studies from Europe have suggested that in some cases chemo may not be needed to continue as previously thought. It is also one of the successes of paediatric oncology with long term survival above 90% for localized disease and 75% for metastatic disease. Successful management of Wilms’ tumor necessitates meticulous attention to correct staging of the tumor and a collaborative effort between paediatric oncologists, specialist surgeons, radiologists, pathologists and radiation oncologists. The poor outcome for patients with Wilms’ tumor (WT) in developing countries has been predicated on late presentation, poverty and low rate of chemotherapeutic access.